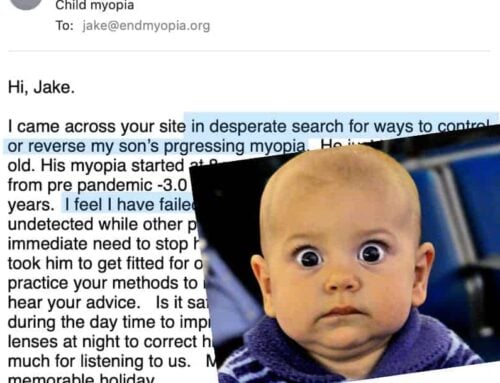
I have a whole category of the blog dedicated to child myopia (link to child myopia subjects).
We can’t apply all the adult strategies verbatim, since there is a big difference between most children, vs. adults: the child might not really so much care about sacrificing short term convenience, for long term gain. In fact, it is quite unlikely for most children, especially in the more vulnerable to eyesight change younger years, to be uncomfortable, for the promise of some future benefit.
You will probably gladly wear a Peak Prescription that barely get’s you to 20/40, and work to clear up your double vision. This is not only more complex for a child to relate to conceptually, and also just isn’t so much fun.
So, for most children (and I mean 12 and younger, in most cases), we compromise on some of the quick improvement opportunities, for the sake of maintaining trust, reducing the risk for the child rejecting the practice, and take a longer term view on eliminating myopia.
In general terms, if you have done or are doing the adult program, taking care of your child’s eyes means some adjustment in priorities. We really want to enforce the close-up distance, and limiting close-up focus. We want to make sure ambient lighting is always good, and that we encourage outdoor play, and activities not involving fixed, close-up focus (playing with legos, vs. playing a computer game).
More focus on reducing strain, and accepting less stimulus, is the premise of child myopia rehabilitation. We have lots of time, and the first thing we want to make sure of, is that we reduce the thing that causes myopia.
I generally recommend a much more nuanced approach to normalized prescription, for children. We want the child to see 20/20, on a well lit Snellen, being able to read about half of the line. If it’s all of it, if we get 20/15, the prescription is too strong. Just at the edge of 20/20, on a correctly done Snellen, allowing the child to see clearly.
If you give the child a 20/40 prescription, the frustration will be too significant, especially when you combine with enforcing close-up rules, having another pair of glasses for close-up vision, and limiting close-up time. We have to compromise.
Number one concern, is to stop your child’s myopia progression.
That is more than half the battle. Even if you get an improvement of just 0.25 diopters a year past that, you are absolutely accomplishing the goal of protecting the child’s eyesight. Little, tiny, below the radar adjustments, is the strategy to deal with child myopia.
Getting the child to not wear that minus prescription distance lens when focused up close, is of course the other big piece of eliminating myopia progression.
Recognize how big the gap is between what you would want for your own eyesight, vs. what your child is interested in. Realize that your drive, your concern, your willingness to put in lots of work, may not be mirrored in your child. Too much pressure, too much dissonance there, will lead to systemic rejection on part of the child. And all the things that make up stimulus, active focus, pushing distance, have to be voluntary. Desire is important there. So even if you have to wait a year or two, for the child to be interested in that, you can today work on limiting close-up strain, and planting the seeds.
Instead of driving for gains today, take the long term view. I even had some clients who would tell their child that he/she could not do some activities until their next birthday. A long delay, but building that desire in the child, taking a bit of a strategic approach to ultimately get the healthy vision, you desire for your children.
Enjoy!