This, an important question, that comes up every so often and likely will be relevant to you:
Should I reduce the prescription strength for my weak eye, to force it to work harder and catch up?
You likely noticed this with your centimeter measurements – one of your eyes is stronger / can see further, than the other. This is entirely normal. It relates to a phenomenon often referred to as ocular dominance, in vision sciences:
![]() The role which the dominant eye plays in ocular functions is as yet not fully determined. Although it has been recognized as being present, ophthalmologists have been indifferent as to its importance and the part it plays in maintaining normally coordinating eyes. The dominant eye may be defined as that eye which performs the major function of seeing, being assisted by the less dominant fellow eye. To state it differently, the two eyes do not affect the visual consciousness with equal force. One eye leads the other, and this leading eye is called the dominant eye. Just as the two hands are unequal in response, both from a motor and from a sensory standpoint, so are the eyes. Just as a person may be right handed or left handed, so he may be right eyed or left eyed. (source)”
The role which the dominant eye plays in ocular functions is as yet not fully determined. Although it has been recognized as being present, ophthalmologists have been indifferent as to its importance and the part it plays in maintaining normally coordinating eyes. The dominant eye may be defined as that eye which performs the major function of seeing, being assisted by the less dominant fellow eye. To state it differently, the two eyes do not affect the visual consciousness with equal force. One eye leads the other, and this leading eye is called the dominant eye. Just as the two hands are unequal in response, both from a motor and from a sensory standpoint, so are the eyes. Just as a person may be right handed or left handed, so he may be right eyed or left eyed. (source)”
—
We could talk extensively about this subject, and there are all sorts of interesting tests related to ocular dominance, and determinations that can be made. It’s a bit much for this article, which is intended to simply relate to your prescription glasses.
Here is the problem: You might have too much difference in prescription between your left and right eye.
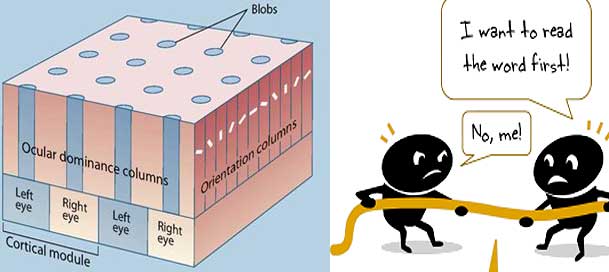
This as with everything else on the myopia subject, isn’t genetic. Rather, it’s what above quote notes, rather ironically: “Although it has been recognized as being present, ophthalmologists have been indifferent as to its importance The optometrist’s *indifference* (often those two go together just a bit too well) is what can increase your natural variance. Say you initially started with with a -1.00 and a -1.25 prescription. With early myopia (NITM), the 0.25 increments are a rather large increment of correction. Your real focusing error might be something like -1.00 and -1.15, for example. Since there isn’t a diopter increment for 0.15, you instead end up with a -0.25 step. And there you have it, the “weaker” eye is overprescribed. What happens next? Lens-induced myopia happens more, on that eye. Your next prescription, if again done aggressively, may again push more prescription on the weaker eye. Lens-induced myopia studies in chicks. It’s a thing! If you spend a lot of time in close-up with that prescription, and you are genetically predisposed to respond strongly to lens induced stimulus, you might end up with a prescription that significantly emphasizes the gap to the dominant eye. In a recent forum post, Cadence mentions: — And there you have exactly what happened, with Cadence. Optometrist indifference, or rather lack of understanding of the realities of lens-induced myopia. The problem you have with this is two-fold: 1) Prescription Complexity: When You Take Off Your Glasses, Your Visual Cortex Gets More Confused Since Left And Right Eye Signals Are Changed. With glasses you get a different set of focal planes than without. In addition to the blur, you get a *different* blur for left and right eye. This makes you even more dependent on glasses than you would be with an equalized prescription. Unfortunately, you can’t just jump to equalized. 2) You Can Loose Depth Perception Entirely. This means, no more depth perception, and increasingly rapid loss of vision participation in the “weaker” eye. It’s not necessarily what happens, but it’s a risk. The higher the variance in left vs. right eye, the stronger the risk. Depth perception test. Do the circles appear to be moving? That’s the issue with prescription. What you’ll be tempted to do is what Cadence is thinking about trying, in the forum – altering the prescription strength for the weaker eye. Alex makes the following observation on this topic: For the first month or two at least, you want to ease into things, not making more than the most necessary changes at one time. By maintaining the same distance in both eyes you are making sure that you are not compromising bifocal vision, and getting the best distance for both eyes. Why? 1. It’s quite difficult to find active focus, when one eye sees more clearly than the other! 2. Combining a prescription reduction with an unequal prescription creates a whole lot of confusion in your brain, where the image signal is processed. We want to avoid this. 3. You want bifocal improvement first and foremost, to introduce the biology to this whole new premise of less strain and more positive stimulus. Yes, we want to concern ourselves with equalizing both eyes, and the course does discuss this later on, when it becomes appropriate (once all the basics are properly covered). At that point we will look at some strategies that are effective, primarily involving patching the strong eye for brief periods of time. That activity builds on what you learned previously, and just leverages active focus with one eye. The main thing you want is a reducing prescription. As long as both eyes improve at the same rate, it’s perfect. When we add a bit of extra stimulus for the higher prescription eye, we help introduce just a bit more challenge to slowly add to an equalizing prescription. — The full thread is here. And that’s the crux of how to deal with this issue. As long as both eyes perform (do active focus), you want to strongly favor bifocal activity and habits, and not worry at all about the difference in prescription strength. As long as both eyes reduce at the same rate, you are in good shape. Once you are well into that process, at least 1-2 prescription reductions in, you can start doing patching and activities Alex outlines in the course. It only makes sense to do so when your eyes and habits are already well used to the process of getting stimulus with bifocal vision. Otherwise it just doesn’t work well and adds unnecessary strain (and demands on your time). Patching. Who says it can’t be done in style? It’s a different story if you already are loosing depth perception because of a significantly unequal prescription. That’s something that the course doesn’t cover and requires some one-on-one time (though you having this problem is statistically unlikely). As always, the forum proves to be an important part of the site and process. Hopefully you are benefitting from these shared insights! Cheers, – Jake —- P.S.: As I look at the incoming new visitor traffic, I notice that all the text heavy focus of the site is not conducive for people’s attention span. In other words, too much writing, not enough incentive to start reading. To that end, I’d like to tell some of the basic myopia story with some animation (and still images thereof). A quick little visual story to explain eye strain, NITM, the first optometrist visit, and then lens-induced progressive myopia. It might help a lot to educate first time visitors! If you have animation skills or otherwise may be able to lend a hand, please do post here in the forum.
![]() I understand that my left eye is much more overpowered by my right eye by around -3 diopters. L- -10.0, R- -7.0. Current normalised glasses prescription is around L- -9.75, R-7.0, astigmatism on both eyes is not much of a concern as they are around -0.50. I was thinking if its possible to get a differential prescription glasses around L- -8.75 and R- -6.50. In this way, I hope to make my right eye work harder as it already became lazy over the years. I need advice if I am actually on the right track.”
I understand that my left eye is much more overpowered by my right eye by around -3 diopters. L- -10.0, R- -7.0. Current normalised glasses prescription is around L- -9.75, R-7.0, astigmatism on both eyes is not much of a concern as they are around -0.50. I was thinking if its possible to get a differential prescription glasses around L- -8.75 and R- -6.50. In this way, I hope to make my right eye work harder as it already became lazy over the years. I need advice if I am actually on the right track.”
![]() It’s a good idea to compare your left and right eye distance either with (or both) Snellen / centimeter, to make sure. You do want a correction that gives you the same distance for both eyes. Here is why:
It’s a good idea to compare your left and right eye distance either with (or both) Snellen / centimeter, to make sure. You do want a correction that gives you the same distance for both eyes. Here is why: