We talk about peripheral vision every so often, here in the blog.
Here’s a quick and possibly startling fact: You don’t use your peripheral vision, when you’re staring at screens. You use only about 3% of your retinal surface, in fact. Is this something you should worry about?
Some clinical science suggests that you may in fact become myopic, because you’re not using your peripheral vision. More on that in a moment.
Peripheral vision falls into the wider category of vision health, and a large part of your eyesight that’s being unnaturally restricted by our modern lifestyles (and wearing of glasses). To be clear right from the start: I have run extensive tests with students and not found that our poor peripheral vision habits explicitly and primarily cause increasing myopia. I won’t tell you that some magical peripheral vision exercise will make or break your long term vision health.
That’s not to say that you should continue ignoring your peripheral vision.
Let’s look at a study titled “Peripheral Vision Can Influence Eye Growth and Refractive Development in Infant Monkeys”, published in NCBI in 2007 (source).
In this study, 12 infant monkeys (12 monkeys, seriously you guys?!)
Remember that movie? Good times …
Anyway. 12 infant monkeys had their peripheral vision obstructed to gauge the impact of peripheral vision on the development of the eye. (for reference, monkey eyes, entirely relevant to human eyes) Here’s the abstract, if science lingo makes you sleepy, skip straight to “conclusions”:
PURPOSE
Given the prominence of central vision in humans, it has been assumed that visual signals from the fovea dominate emmetropization. The purpose of this study was to examine the impact of peripheral vision on emmetropization.
METHODS
Bilateral, peripheral form deprivation was produced in 12 infant monkeys by rearing them with diffusers that had either 4- or 8-mm apertures centered on the pupils of each eye, to allow 24° or 37° of unrestricted central vision, respectively. At the end of the lens-rearing period, an argon laser was used to ablate the fovea in one eye of each of seven monkeys. Subsequently, all the animals were allowed unrestricted vision. Refractive error and axial dimensions were measured along the pupillary axis by retinoscopy and A-scan ultrasonography, respectively. Control data were obtained from 21 normal monkeys and 3 infants reared with binocular plano lenses.
RESULTS
Nine of the 12 treated monkeys had refractive errors that fell outside the 10th- and 90th-percentile limits for the age-matched control subjects, and the average refractive error for the treated animals was more variable and significantly less hyperopic/more myopic (+0.03 ± 2.39 D vs. +2.39 ± 0.92 D). The refractive changes were symmetric in the two eyes of a given animal and axial in nature. After lens removal, all the treated monkeys recovered from the induced refractive errors. No interocular differences in the recovery process were observed in the animals with monocular foveal lesions.
CONCLUSIONS
On the one hand, the peripheral retina can contribute to emmetropizing responses and to ametropias produced by an abnormal visual experience. On the other hand, unrestricted central vision is not sufficient to ensure normal refractive development, and the fovea is not essential for emmetropizing responses.
So what do we learn from this?
Most of the monkeys (9 out of 12) had become measurably myopic from having their peripheral vision restricted. Removing the restriction caused all monkeys to fully recover.
That’s a pretty definitive outcome.
And yet your highly esteemable eye guru Jake VanJakenstein says that you should only concern yourself with peripheral vision, after you deal with core natural myopia control topics like differential prescriptions, blur horizon, active focus, managing eye strain, outdoor time, and keeping a log. In other words, VanDerJaken tells you that despite the 12 monkeys, peripheral vision is tertiary at best, when it comes to improving (or maintaining) your eyesight.
Mostly this is because we start with clinical science, published studies. We read them, review the merit, and then do our own studies. I’ve got my own 12 monkeys (you might be one of them, if you’re in BackTo20/20 and ever were invited to be part of a test group). And unlike any other study, we are focused specifically on vision improvement for human adults, in the real world.
This means that we learn the most about what tangibly matters, and not in a circle-jerk academic publishing scenario. Endmyopia is for you, with limited time and attention span, looking to keep your eyes healthy.
More on peripheral vision and to what extent it matters, in the latest eye guru video on Youtube:

Getting into the monkey business, on the tubes.
Give it a thumbs up, your darling eye guru will have an existential crisis if you don’t. And subscribe to the channel. And Twitter. And Quora. And Instagram. (not really Instagram, unless you want to voyeurize the upcoming shenanigans in Yangon Myanmar, next week).
Housekeeping: Looks like most of the progress logging tool bugs are ironed out. We’ll be phasing it in gradually more and more, to make sure that new students use it consistently. This has been a gigantic f##### headache, cost has run almost into the four figure range (yikes), but it’ll definitely be worth it in the long run.
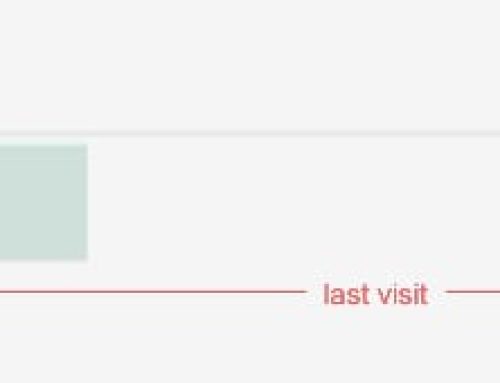
Data is king, with proper science projects. Right now the tool won’t correct automatically for common mistakes (like not putting the minus sign in front of your diopters), so if your log looks a bit weird, just go back and double-check / edit your log:

I’d put zero a few times in my centimeter results and my centimeter chart reflects it. One day the log tool will be smart enough to question that input but for now, no babysitting. ;)
Cheers,
-Jake