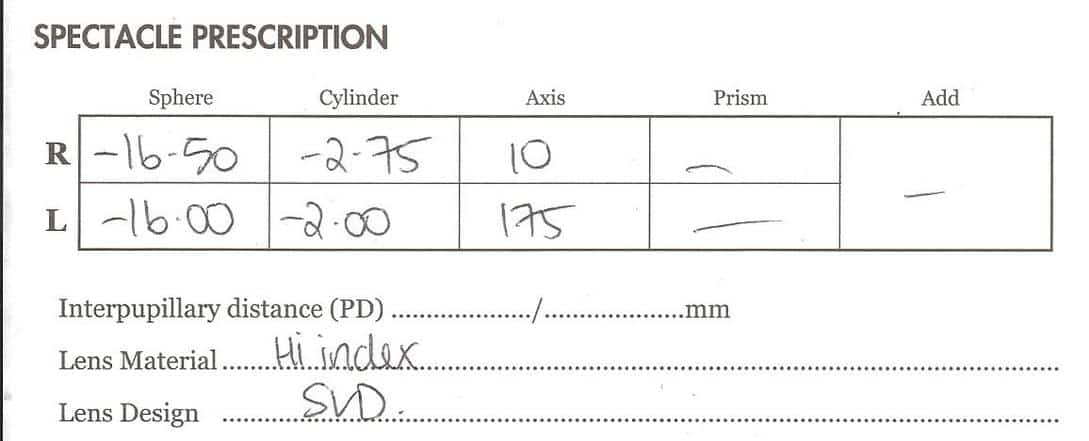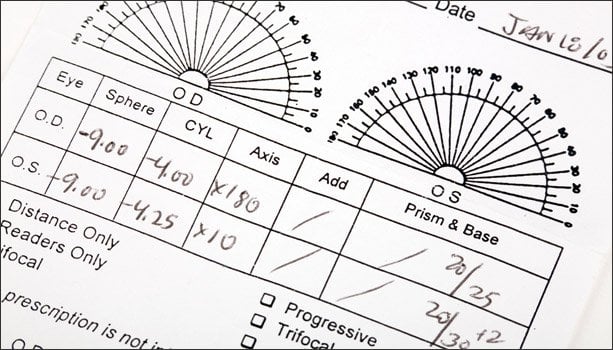
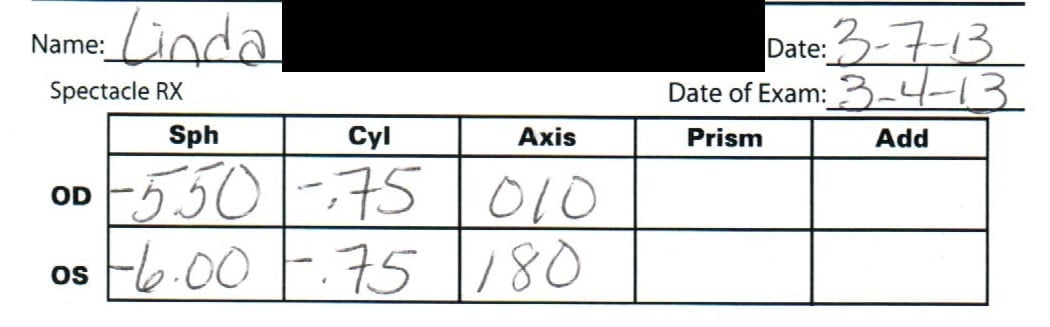
If you ever checked your prescription, you might have noticed this:
The left eye diopter numbers are different from the right eye diopter numbers. Do you know why this is? Is it because your left eye is actually not seeing as well as your right eye (or vice versa)? Is there something wrong with the balance between your eyes, that the magic of optometry helps correct?
Time to break out nope-cat for this one:
Every human being who has two eyeballs (some pirates excluded), has one dominant eye. You’d never even notice this, since your bifocal vision and depth perception works just fine. It’s just that if you measure very carefully (darkened room, Snellen eye chart, single eye tests), you’d notice a small difference between left and right eye. This is perfectly normal and the case for just about everyone. Science doesn’t know exactly why, but science knows that it is the case. This is important. Science, knows.
Here’s where the problem starts.
You go to the optometrist and in the zeal to dope you up on as many unholy minus diopters that they can possibly jack you up on, the optometrist discovers a “weaker” eye. Your eye chakra is weak, son.
I’m just one good acid trip or failed paragliding experiment away from being too weird to write this blog.
Anywho. You have a dominant eye, which the optometrist will end up giving a little less prescription to, than your “weaker” eye (which is in fact biological design, not some kind of failure). As we know by now, lens-induced progressive myopia now happens due to the stimulus created by the minus, and your eyes will adapt to the prescription. The unequal prescription. Which, unsurprisingly, is likely to get more unequal as your myopia increases. This because of optometry interference and prescription zeal, not because some biological flaw in your vision.
10% diopter ratio. Normal, though not necessary.
The most ironic bit here is that your darling best friend Jake is the only one (or one of the rather very few), and not an optometrist no less, to be able to explain this to you. You’re having to resort to the mad hippie ex banker, to get answers to myopia questions.
(The air con in this coffee shop is so cold, my fingers are about frozen. Possibly this, the cause of today’s slightly more odd than usual tone.)
Resist getting a diopter ratio prescription that favors a “weak” eye.
Now if you already have a really pronounced diopter ratio, you can’t just reset the clock. You don’t want to get all hung up on equalizing (what we call this here). Reducing your diopter dependence (bifocal) is what you want to focus on, not equalizing. But it bears knowing where it all comes from anyway. And we do of course discuss in BackTo20/20, at the right time, how to reverse that ratio, gradually and effectively.
This post today, because of two comments I left in the forum in response to student question.
One I found changing diopter ratios for different lens wear scenarios. That’s something we absolutely, positively, always want to avoid:
Important first point: The diopter ratio needs to stay the same throughout the prescription range. So whether you wear full, normalized, or differential, the difference between left and right eye diopter shouldn’t ever change.
If I understood correctly, your differential solution, the reading glasses, don’t follow that rule. Need to fix that, first and foremost. Very important.
Second, again if I get this right, you decided to normalize your distance prescription with the -7 for left and right eye. While the result sounds perfectly suitable (slightly faster dominant eye is normal), I’m not sure whether there are still other diopter ratios in play. If so, very important to eliminate these variations in diopter ratio.
One ratio throughout the range. If you mess with this, you’re going to get all sorts of inconsistent results and issues with your visual cortex processing the signal correctly. Headaches, lacking progress, all sorts of unwanted side effects can happen there.
If equalized (same left and right eye diopter) is close enough with centimeter (which by what you are describing may be the case), then just go equalized all the way around. If not, still be sure to maintain the ratio.
Let’s make sure that’s the case, so going forward things will go smoothly. ?
Don’t mess with the ratio.
Until you’re well into several successful bifocal, equal diopter reductions, that’s a no-no. Also perfectly all right to not have known that, and ask questions in the forum, so I can catch these things early.
On another question, I comment on the difference between perceived better vision in one eye over the other right now, vs the longer term aspect of actually improving vision (which tends not to exhibit actual difference in left and right eye rate of improvement):
It’s always like that, dominant eye resolving faster. As long as the centimeter results improve at about the same rate, it’s just what you might expect.
A lot of times I’ll say to just keep reducing the diopters while maintaining the ratio. But since you’ve been at it for a while, making good progress, sometimes it’s helpful to incorporate a little equalizing with giving the “weaker” eye a break. Generally you don’t want to favor it (that’s what leads to those big ratio prescriptions in the first place), but after a series of equal ratio reductions, one of these equalizing changes is ok.
After everything adjusts, you’ll eventually find the same thing happening again, with the dominant eye resolving faster – though not actually improving faster. There’s the difference between the immediate perceived vision (clear flashes, blur horizon clearing) and the longer term improvement (ie. centimeters). You tend to get the dominant eye resolving faster right now, but over time the centimeter changes should be fairly equal for both eyes.
Make sense?
Keep an eye on left and right eye centimeters. Make sure that both improve at the same rate. Wear lenses that give you about the same centimeter left and right, without favoring one eye. Ask in the forum, if you aren’t sure.
Cheers,
-Jake
P.S.: Can’t get enough of these awesome posts? Want more details and off-topics, and what I’m jamming to while writing your guides, and travel updates (day after tomorrow, find me in Singapore!), and getting all hippie with live kefir grains? Follow me on the Twitters.
PP.S.: If you’ve got one of these, best start researching where you want to get emergency retinal detachment surgery. Yikes.