Most of us don’t care about our health, as long as we have it. Prevention isn’t high on the list. Not for me, and probably not for you. When we talk about myopia as a problem with potentially unfortunate consequences, most people nod and move on to check their Facebook updates.
But should they. You want to wait till you are looking at lens implants as a way to keep your eyesight? Well, maybe you ought not to …
—
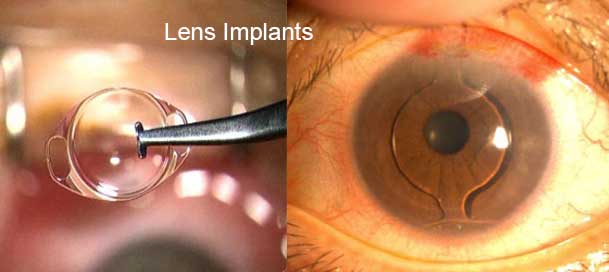
Lens implants (IOLs) are a growingly popular staple in the surgeon’s stable of product sales vision therapies. These things have been around for a long time, through periods where the establishment was fondly using the term, close enough.
If you let your eyesight health go down the drain far enough, eventually you may encounter the possibility for having lenses implanted in your eye. What’s one of the keys to success for that procedure? Measuring your eye first (axial length).
Let’s indulge in a tale from Ophthalmology Management magazine, in parts, for this article:
“In the early days of IOL implantation prior to commercially available biometers, the accepted strategy for achieving emmetropia with a posterior chamber IOL was simply to add +18.0 D to the preoperative refraction. Equally primitive were the early IOL power calculation formulas, which often produced large refractive errors for long and short eyes.”
Large refractive errors. Primitive.
In all fairness, a lot of that above was 40 years ago. If you were unfortunate enough to walk into one of those guys’ office back then, that’s what you would have gotten.
But things have changed! Today, your odds are far, far better.
“Forty years later, both technology and patient expectations have progressed dramatically. Gone are the days when just being close to the refractive target was good enough. For a cataract surgeon implanting presbyopia-correcting IOLs, one important part of the procedure’s overall success requires accurate preoperative measurement of axial length.”
Progressed dramatically. You should feel reassured, especially if you are having to consider IOL for keeping your eyesight. Except, for, you best get well aquatinted with surgical procedures, and measurement systems used by your medical professional:
“Applanation, or contact, biometry begins by placing the ultrasound probe directly on the corneal surface. Even the most experienced technician may encounter parallax problems, causing a measurement that’s off-axis by small or large amounts.
When attempting to center the probe on the cornea, there will always be some degree of corneal compression, especially for patients with reduced intraocular pressure. It is this unavoidable artifact of variable corneal compression that generally makes the applanation technique inadequate for the accuracy required for presbyopia-correcting IOLs.”
“Even the most experienced technician” (cue the bad things about to happen background soundtrack), may encounter … oops. Sounds of dropped scalpels and broken glass, out of the line of your sight. Oh don’t worry Mr. Jones, we weren’t using any of those.
40 years have gotten us a long way, but not past “unavoidable artifacts” and “technically inadequate”.
Why all this talk about eye measuring and IOLs? Because you need to take care of your eyes, before you wind up reading an article like this not just for idle entertainment. There could be the day where you read something like this, and seriously have to be curious about applanation measuring techniques. Because you’ll be worried about not being able to see after they’re done with you.
Relevance? Yes, applanation is being called inadequate. But that doesn’t make it obsolete.
Applanation is still a thing being sold, promoted, and trained on (like, here). You can ask one guy and he’ll tell you the thing is outdated and inadequate, or another guy who happens to have his research funded by Zeiss who’ll tell you that it’s just great, fantastic, perfectly good enough (though the applanation method in that study was used as control mechanism).
On the topic of measuring for IOLs, you might be interested in immersion ultrasound and optical coherence biometry:
“Even as reliable as immersion ultrasound has been, clinicians have increasingly used optical coherence biometry for intraocular lens calculations. Minimal patient cooperation is necessary for optical biometry, which can be performed in the fully upright position by technicians with adequate training. Software and hardware have advanced significantly in recent years. The Carl Zeiss IOL Master uses 780-nm light to measure the distance from the retinal pigment epithelium to the corneal surface. It’s quick, accurate, and doesn’t require contact with the corneal surface.”
If you are ever going to end up looking at IOLs, you’ll want to be pretty well educated about the procedure. Which you shouldn’t imagine you’d have to be, shopping ophthalmology practices like you would your next car.
You don’t want to end up in these guys offices. Probably pretty obvious, just having read this article. They are a great solution if you are having an acute problem. But counting on them as a good idea for down the road?
Perhaps it’s just better to take care of your eyesight today.
Cheers,
– Jake