Today has been surprisingly light on e-mail, leaving a bit of time for a quick post here for you. One of the e-mails I did receive today, asked about axial elongation – and the invariable quote from some professional or another that axial elongation is irreversible.
First of, axial elongation of the eyeball isn’t something to think about a whole lot, until you are well past -6 diopters in prescription.
I have seen many hundreds of cases well into the high 5 diopter range, without any axial elongation. Likewise, you could be at -8 diopters, and have no more than a single millimeter of axial elongation (for reference, your eyeball is about 25mm long). Of course axial elongation can become a serious problem, and lead to retinal detachment and blindness. This is something though to worry about in high myopia cases, and even there we can do a lot to drastically reduce the risk.
Back to the point though, about this ostensibly irreversible axial elongation.
What causes axial elongation? It is of course, the use of prescription lenses and the resulting lens induced myopia. Lenses which were prescribed and recommended as treatment plans by the very same individuals who now tell you that the resulting axial elongation is irreversible.
There are a few ways to look at whether axial elongation is irreversible, or not:
1. The Human Body, Responding To Stimulus
This is the least scientific of the options I present to you here. Still, let’s start by considering some interesting things:
Why does the eyeball elongate? It does so in response to stimulus. The stimulus being that big minus lens which moves the focal point inside your eye. That part, a 30 second Google Scholarly inquiry (and more on that in a moment). Of course even this is not clear to some in the optometry business, even though it’s a well established finding.
What else in the body responds to stimulus? How about the gym: you go lift heavy weights, your muscles increase in size. What happens when you stop? Do you remain as muscular? If the new stimulus is sitting on the couch and watching TV, your body will adapt to it, reversing your muscle mass to some extent.
This thought exercise can be applied to many stimulus response aspects of the human body, and of course it also applies in the case of axial elongation. Then, looking at it from just a common sense angle – why would the eyeball be an exception to the rule of stimulus?
But of course this is just philosophical. Let’s look at another way to dispel this notion of irreversible axial elongation:
2. Hundreds Of Cases Of Reversed Elongation
I have seen it more times than I can remember, and we stopped actually testing for axial elongation for many standard cases as long as 15 years ago. The result always being the same, and the test needlessly incurring cost for the client, it just made more sense to forego it.
But that’s just me telling you that I have seen axial elongation reversed as predictably as sitting on the couch and eating pizza didn’t help my jogging abilities.
In this same spirit, you can try it yourself. Of course this take times, but it’s the only way that truly matters. If you are worried about axial elongation, and have an elongated eye, reading about whether it is or isn’t possible won’t change your problem. The only thing that will change it, is to embark on the adventure of some healthier eyesight habits, and proving to yourself that it is possible.
That’s all that matters in the end, and it’s the reason you don’t find my abstract science philosophy talk and endless study references on this site – I want you to spend time proving to yourself what’s possible, rather than getting caught up in pointless arguments for and against myopia rehabilitation.
Still, you might be looking for motivation to actually go try it yourself. So, let’s look at yet another way:
3. Science Shows That Axial Change Happens In Both Directions
First and dispelling the rumor that the eye only elongates and never shortens – axial length tends to reduce with age.
This is somewhat common knowledge, that your distance eyesight tends to improve a bit with age. Or, as many studies to the effect investigate, such as this one:
Reduction in axial length with age: an emmetropizing mechanism for the adult eye?
“Included in the analysis are component data for one eye of each of 271 subjects from age 4 to age 70 years, whose ocular refraction was between plano and +2.00 D. The results of this analysis show that the axial length of the eye appears to decrease during the adult years of life, concurrently with a decrease in anterior chamber depth and an increase in the refractive power of both the cornea and the lens. It is proposed that a reduction in the axial length of the adult eye serves as an emmetropizing mechanism, occurring in harmony with the increase in the refracting power of the eye, which would otherwise cause the refraction of the eye to move in the myopic direction.”
Original article, here.
As usual, these things don’t make for exciting reads. Also, they contain dangerous, if not heretic words like “emmetropizing mechanism” which dare suggest that the eye is actively participating in proving you with clear vision. This of course goes counter to the retail optometry doctrine, that your eye is just a dumb sphere that must be fixed with glasses.
If you do a bit of searching in these studies, you find a lot of intriguing notions that should fuel your desire to go work on your own eyesight. In the one above, I particular like this sentence:
“ It is proposed that a reduction in the axial length of the adult eye serves as an emmetropizing mechanism.”
You will find this quite a bit, and of course throughout this site we often refer to positive stimulus – which in applied practice is more meaningful to you than a lot of these studies. I call it positive stimulus, as it is the challenge to focus that we create with my method that creates the eyesight improvements you are seeking.
There is a rather wide range of these studies, and they all speak a far more logical language than most of the retail practitioners, optometrists and ophthalmologists alike:
Homeostasis of Eye Growth and the Question of Myopia
That’s the title of a rather lengthy article on Sciencedirect.com, with many references that your friendly eyeglass sales professional would find deeply offensive. Let’s take just a few choice references:
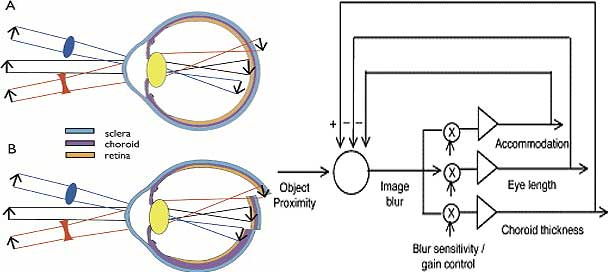
“Control of Eye Growth by Visual Signals
Spectacle Lens Compensation. The homeostatic control of eye growth functions to keep images sharply focused on the retina. Therefore, if the eye length increases more slowly than does the focal length, the focal plane will be behind the retina, creating hyperopic defocus on the retina. The same occurs if one puts a negative lens over the eye (Figure 2A). To regain sharp focus, the retina needs to be displaced backward to where the image is. This is done in two ways: the eye is lengthened by increasing the rate of growth or of remodeling of the sclera at the posterior pole of the eye Gentle and McBrien 1999 and Nickla et al. 1997, and the retina is pulled back within the eye by the thinning of the choroid, the vascular layer between the retina and sclera ( Figure 2B; Wallman et al. 1995 and Wildsoet and Wallman 1995); once distant images are again focused on the retina (emmetropia), both the rate of ocular elongation and the choroid thickness return to normal.”
The eye is lengthened as effect of the minus lens. We did already know this.
However, this particular article, the likes of which you can easily find yourself via a quick search on Google Scholar, is full of interesting insights on the change of eyeball length:
“The beauty of studying the homeostatic control of eye growth is that because it is strongly guided by visual error signals, we can manipulate it in ways that would be difficult or impossible with other organs. For example, the set-point about which the eye growth is regulated can be precisely controlled by the power of the imposed spectacle lens, thereby arranging for homeostatic maintenance of different eye sizes. Furthermore, increases and decreases in size can both be studied within a single animal by fitting different spectacle lenses to each eye. Finally, the temporal aspects of the feedback control can be studied by manipulating the timing of the error signals by putting on and off a spectacle lens.”
Those are compelling ideas, yes?
“Increases and decreases in size can both be studied within a single animal…”.
It is a carefully composed review of a number of well known studies, looking at causes of myopia, and the eyes ability to adjust it’s length according to environmental stimulus. And while the discussion is more about the effect of lenses and other stimuli, there are a number of references discussing that ocular growth is the eye’s participation in environmental stimulus, rather than some abstract genetic defect.
The article concludes:
From the point of view of homeostatic growth control, we have shown that the growth of eyes is guided by vision and probably by subtle computations on the visual input, in animals as divergent as fish, birds, rodents, and monkeys. Because the visual error signals can be easily manipulated, the homeostatic growth control mechanism of the eye may be decipherable, providing a useful model for the study of size control of other organs.
That eyes control their growth by visual homeostatic mechanisms is shown by the rapid compensation for the defocusing effects of either positive or negative lenses, although the mechanisms and temporal properties of compensation in the two directions are different. For example, briefly wearing a positive lens or removing a negative lens can cancel day-long wearing of a negative lens in both birds and mammals. The homeostatic controller corrects the defocus by appropriate modulation of the choroidal thickness and of the rate of ocular elongation, although the two can be decoupled to some extent. Visual deprivation also causes myopia, but probably by a different mechanism.
With respect to human myopia, the importance of environmental factors such as educational level argues against viewing human myopia primarily as a genetic disorder or a disease. Instead, the question might be better phrased as: what aspects of ocular homeostasis are associated with myopia? Long periods of reading might defeat the cancellation of blur from distant objects by blur from near ones, and this might drive the set-point in the myopic direction; the temporal pattern of reading may also influence whether myopia develops. Also, accommodation and emmetropization might be weakened by blur adaptation. Finally, the homeostatic control of refractive error appears to be exerted over a broad region of the posterior globe, averaging, for example, myopia in the central retina together with hyperopia in the peripheral retina. Our limiting attention to central vision may prove to have been a myopia in itself.
For the whole, rather lengthy abstract, visit here: http://www.sciencedirect.com/science/article/pii/S0896627304004933
***
Conclusion, As It Is Relevant To You
Don’t worry about axial elongation, as a roadblock to your eyesight improvement.
There are many studies and discussions like the ones I mention above, all going back to axial change, as it occurs in both directions in the eye. Your eye is actively participating in seeking clear vision. Your glasses are confusing this process, as they might be providing far more focal correction than is appropriate. Your close-up habits, 8+ hours per day in front of a computer, may be providing stimulus that is taking your eyes in the entirely wrong direction.
All these things can be corrected, by you, in small, simple steps. The forum is full of accounts of this in progress. Science is full of supporting evidence that you are on the right track, by seeking healthier eyesight from engagement in the process, rather than just relying on corrective lenses.
And in the end, it’s all just philosophizing until you actually participate and experience your own improvement!