A Detached Retina Has Three Common Causes
-
- High degree of myopia (near sightedness)
- Eye injury or cataract surgery
- Genetic / family history
Retinal tears happen before detachment, usually, with symptoms including seeing ‘floaters’ (specks of light), flashes of light, and potentially darkening of your peripheral vision.
If you experience any of these symptoms, you want to see a doctor immediately. Every minute counts, since only very quickly executed surgery can re-attach your retina. You absolutely do not want to delay getting these symptoms checked.
***
The Real Tragedy About Retinal Detachment Is That It Can Often Be Prevented.
Disclaimer: Go see an ophthalmologist if you have any doubt or questions or are at risk of retinal detachment. Never, ever look at any Internet monkey for advice on serious medical conditions. Seriously. This article, just for exploring some of the scientific evidence and discussion related to this topic.
Out of the causes above, three are fairly rare. Let’s take a look:
Eye Injury
While an eye injury can cause retinal detachment, it is highly unlikely – and if it does happen, you will be seeking immediate medical treatment anyway. This one isn’t one we would sit and read this article, and worry about.
Cataract Surgery
Cataract surgery, indeed can have this side effect – though it most likely will not, especially if you are not also highly myopic. We will get to the why of that, in a minute.
Family History
Family history likewise, is a secondary cause. For it to become a tangible risk, you need a catalyst. Which could be an eye injury, or high myopia.
High Myopia
This is where we start having the problem. How do you know if you are at risk? Let’s take a very quick look at how myopia can become the catalyst for retinal detachment (especially if you have any of the secondary risk factors, listed above, already against you):
All Myopia Is Made Up Of Two Components: NITM and Lens Induced
NITM
Near work induced transient myopia (see Google Scholarly results) is the root cause of almost all myopia. It is well documented in medical science, in countless published studies over the past 40 years.
It is the first bit of myopia, up to -1.5 diopters, which simply comes from too much reading or computer work.
It’s how myopia starts.
The problem with NITM is how it progresses – once you add glasses to the equation:
Lens Induced Myopia
Equally well known to medical science (see Google Scholarly results), this is what happens when you correct that transient (meaning, temporary!) -1.5 diopter myopia, with prescription lenses.
Every single study (see link above for hundreds of them) shows that wearing a minus lens will increase the myopia degree, and change it from a temporary symptom (NITM) to a more permanent, and more dangerous one (lens induced).
How does this relate to retinal detachment?
Lens Induced Myopia Can Cause A Lengthening Of Your Eyeball.
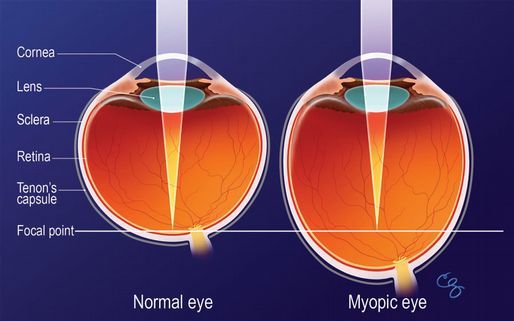
Above – the eyeball growing longer with increasing myopia.
Especially as you get into higher myopia, past -6 diopters, your eyeball is becoming more egg shaped, than round-ball shaped. 3 diopters equals about 1 millimeter of elongation – up to -6 diopters you may actually have no elongation at all (if you are lucky), but past that, your eyeball is definitely getting longer.
This is entirely caused by the lens, your glasses (lens induced myopia).
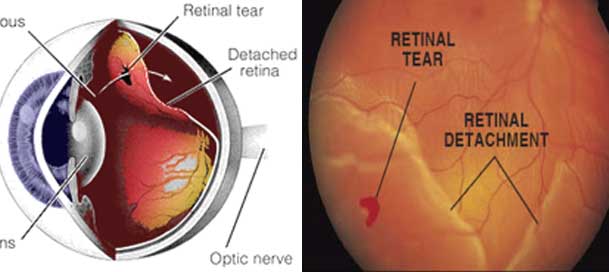
The Elongation Of Your Eyeball Strains The Attachment Of Your Retina.
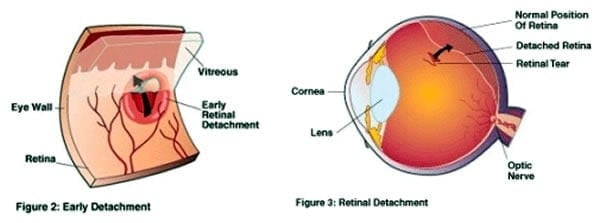
Above – the attachment of the retina is strained until it detaches.
Since the retina is attached to the inside of your eyeball, and is of a different density, your elongating eyeball starts squeezing the retina (as it is getting more egg shaped, there is less space for the retina, it is being squeezed forward along the walls of your eyeball).
Now there is stress on the attachment of the retina. All day, every day, that attachment has to fight to keep your retina attached to the eyeball.
Of course if you now add trauma (an eye injury or surgery), or a hereditary weakness in the attachment to this dangerous equation, you might start seeing floaters, or any of the other alarming symptoms of the attachment beginning to fail. And eventually, you could end up with a detached retina.
***
A Detached Retina May Be Prevented, By Not Allowing Progressive Myopia To Happen.
Take away the eyeball elongation, and the risk for a detached retina becomes infinitely smaller.
You do of course need to wear glasses, if you are highly myopic. But the extent to which you use how much correction, is a whole different story. The key concept of the blur horizon help drastically reduce the impact of lens induced myopia. Using an appropriately lowered prescription for all of your close-up work, and avoiding overprescription will help reduce eyeball elongation.
For myopia degrees over -10 especially, working on reducing that myopia, will also reduce retinal detachment risk.
Lots of mainstream practitioners will tell you that this is impossible. They will tell you that anything besides their advice (which is, sit and wait and hope for the best), is quackery. Arguing with them is of course, fruitless. Even though you might be tempted to refer to the many studies you may have read (see Google Scholarly links above), that clearly demonstrate NITM –> Lens Induced, and the consequences of axial elongation.
The same professionals who prescribed the “myopia treatment” that caused your lens induced myopia, which in turn hugely increases the risk of blindness from retinal detachment, tell you that you can’t do anything about it.
For them to say anything else, would not only obviously imply malpractice, but would also upset the whole dogma of fixing all myopia with glasses. If you look at the lens induced studies, you will also find more than a few that show that the axial elongation tends to reverse, without the lenses in place. And while this is not something we can do by “quitting cold turkey”, a planned and monitored ongoing reduction of correction is entirely feasible. See the vision improvement course and client reviews for more on the subject.
Let me end this article with a quote, from the British Journal of Opthalmology:
 Ophthalmologists should also recognise and take up the challenge of preventing or curing myopia by addressing its cause and not simply treating the consequences.”
Ophthalmologists should also recognise and take up the challenge of preventing or curing myopia by addressing its cause and not simply treating the consequences.”
(Full article) That’s for all of the experts, doctors and optometrists, who tell you that there is no cure or prevention, and that the cause of myopia is unknown.
Unknown to them, perhaps.
But not unknown to science. And apparently, not unknown to the foremost medical journals they should be reading. Take care of your eyesight, be careful of overprescription, and follow basic concepts of healthy eyesight to reduce your risk of a detached retina.