In the Web Program you find me suggesting that you use no less than three different ways to measure (and track!) your eyesight, and vision improvements. We have a close-up test, and two distance tests as core measurements, all telling part of the story.
This is more of a casual visitor story, if you have done the program, all of this is familiar to you already.
You want to check your eyesight both for long term motivation, as well as to help identify which practices may be most effective – as each individual responds a bit differently, to various stimuli. If you are the type of person who does not like to measure and track, but feel completely confident in your ability to continue you, you could even skip the tracking process. I don’t recommend it though, at least not for the first six months at least.
This lies in stark contrast of how your eyesight is measured at the optic shop, where they take a single round of measurements by which your prescription is determined. This is a problematic practice, at best.
We will get to the Yeti, in a moment. First though, let’s take a closer look at this most common way that eyesight is checked:
The Eye Chart
This one everybody knows. It is what you get tested on at the opticians shop, and in the Web Program one of my first recommendations is that you buy or print one, for home use as well.
It is the first out of two ways we look at distance vision.
If you are new to the site, it bears mentioning that this test is not accurate, as a single measurement. That is to say, if you go to the optometrist, and you get your eyes checked, you get a single snapshot from what is actually a fairly wide range.
Because a) your eyesight is quite variable (based on external factors, as well as your habits), and b) the eye chart can be presented in quite a few ways.
Let’s look at a recent forum comment, on the subject:
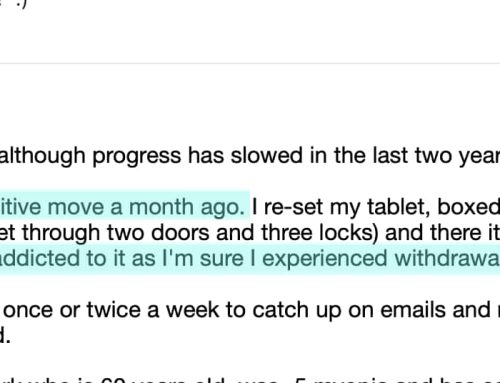
![]() At the optician it surprised me to find out that their idea of clear vision is much above 20/20. At home I can get 20/20 vision with a -1,5 prescription during the day, even when it is cloudy(this used to be a problem, so definitely an improvement here). At the optician I was able to read every line with a -1,75 prescription, but he would prescribe me -2, solely because -2 was a small improvement from -1,75. Another thing is the contrast on the chart. My own chart has clear black text on a white background, the one at my optician was grey/beige
At the optician it surprised me to find out that their idea of clear vision is much above 20/20. At home I can get 20/20 vision with a -1,5 prescription during the day, even when it is cloudy(this used to be a problem, so definitely an improvement here). At the optician I was able to read every line with a -1,75 prescription, but he would prescribe me -2, solely because -2 was a small improvement from -1,75. Another thing is the contrast on the chart. My own chart has clear black text on a white background, the one at my optician was grey/beige
(The full thread is here.)
So here we have an individual, who checks his own eyesight. He can see 20/20 with a -1.50 prescription lens (in most average, day to day scenarios).
The optician, however, wants to prescribe a 25% higher correction, than appears necessary. Why risk Andreas long term eyesight health, with this 25%? It more than likely, after all, will lead to the progressive myopia symptom that most people experience, after their first glasses are prescribed.
Now before anything else, the optician is not wrong. This is a bit of an industry standard, prescribing to the very limit, because: the 25% excessive prescription accounts for the worst case scenario.
If Andreas were to need the prescription at night, in a foggy snowstorm, to drive at high speeds on the highway in Germany, he would definitely want that -2 diopters to give him the absolute maximum clarity. Allowing that Andreas may decide to go Yeti hunting in the Austrian Alps, at 4am, in dark, dense forests, amongst mysteriously swirling misty fog, correcting to the very limit is good insurance for the optic shop. Andreas won’t be able to complain that he missed his target, due to weak glasses.
But, on an average day, take a bus to the office, do some work, go out for lunch, -1.5 is more than adequate. -1.5 is 20/20 in non-Yeti conditions, for Andreas.
This all goes back to why the single prescription paradigm invariably leads to more myopia.
Changing the focal plane, the way light reaches the retina inside your eye, by an additional 25%, is a massive dose of change. It sounds small in numbers, at a -1.5. But if you are at -4, then 25% is suddenly quite a bit of diopter. And even on the small end, 25% is just about guaranteed to have all sorts of myopia inducing effects on Andreas eyes.
Of course, if the optometrist told Andreas to never wear these glasses while reading or working on the computer, and to only wear them when he was outdoors at night, possibly Yeti-hunting in swirling mist Austrian forests, focused on distant shadowy creatures, the negative effects would be far, far less severe.
But that isn’t the case. We get the maximum dose of focal plane change, and are told to wear them all the time. And that, in no small part, is how myopia has come to affect untold millions of people, just in very recent times.
Let’s get back to the point, though:
Learn to measure your own eyesight, and learn exactly what it means.
- As Andreas correctly assesses, a beige background Snellen won’t give you the same results as a white on black Snellen.
- A fully lit room Snellen test will give you a different result, than a dark room, spot-lit Snellen.
- Late in the day, after work Snellen, different result than fresh, in the morning Snellen.
- Natural light Snellen, different result than limited UV spectrum Snellen.
- After eating a big meal full of carbs, different Snellen result than on an empty stomach.
You get the idea.
So to fully understand your eyesight, you will want to measure up-close (the centimeter calculator, which you can find here), and measure at a distance. You want to look at a Snellen chart, in various conditions (as listed above). You will also want to do reference object measurements, as described in the program. While that form of measurement does not give you a specific value at that time, it will tell you how your eyesight changes over time (a result, which may vary from what you find from centimeter or Snellen).
It isn’t until you have a range of results, that you have an accurate insight as to what degree of myopia symptom you may want to correct.
And of course, single prescription paradigm is a recipe for eyesight disaster. Just as we wouldn’t take morphine for a headache (however indisputably effective it might be, at curing the symptom), we don’t want to use the maximum amount of dangerous focal plane change, for all waking hours.
Remember the special winter eyesight improvement installments, now just around the corner!
As always … enjoy!
![]()