A contact lens, specifically marketed to children, said to prevent high myopia?
Coopervison MiSight contact lenses present a complete paradigm shift in commercial, mainstream myopia control. They should be making news worldwide for their break with tradition, and wild claims that focal planes affect myopia development.
But nobody is really talking about them. Why?
Let’s take a look at what Coopervision claims with their MiSight contact lenses:
“Reduces Myopia Progression”
“Reduces myopic progression, for better vision when not wearing glasses or contact lenses”
This quote is taken directly from Coopervision’s MiSight marketing materials.
That’s a bold claim, as much of mainstream optometry still lives under the “myopia progression is beyond our control” rock. It’s the first line item of Coopervision’s claims no less, a straight shot at the bow of the “myopia is genetic” apologists that define much of the mainstream myopia camp.
Can a contact lens reduce myopia progression?
The big one is yet to come on this front, since this is no Ortho-K, no lens reshaping, but a much more interesting approach to myopia control.
Let’s look more at the marketing claims, first:
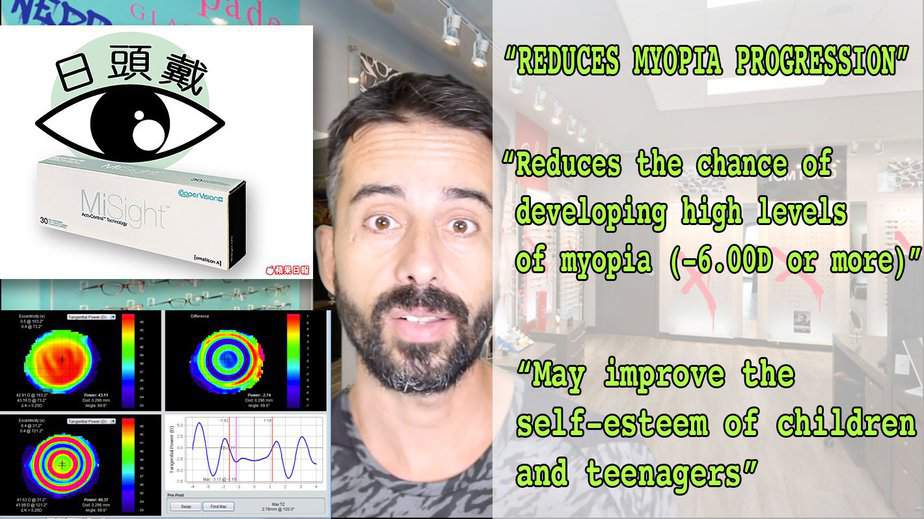
“Reduces the chance of developing high levels of myopia (-6.00D or more)”
” … which may lower the incidence of eye diseases associated with short-sightedness such as retinal detachment and glaucoma.”
Another big one here.
While it’d be more fun to hold out with the bit of how they claim to accomplish this, it’s time to reveal their mystery ingredient that’s supposed to make all this possible. After all, we’re talking about a contact lens said to be able to prevent high myopia altogether, which is a bold claim.
Let’s use a visual straight from their marketing materials:
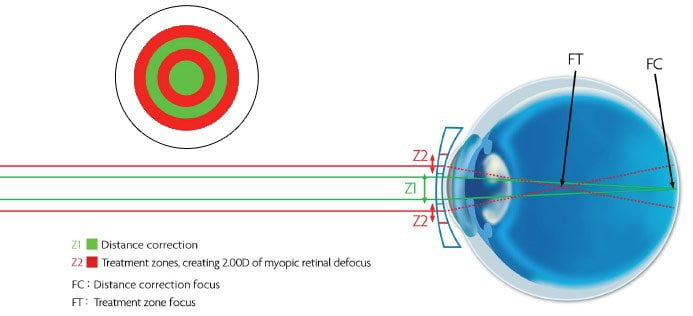
Take a moment to marvel at this one.
They are using 2 diopters of strategic myopic defocus, separate from distance correction focus, to reduce myopia progression.
This is nothing less than heresy, on the level of retail optometry.
Optometrists all over the world are still being threatened with having their license revoked, for merely suggesting the possibility that myopia progression can be reduced or stopped. Much of the mainstream staunchly believes that focal planes have nothing to do with myopia progression, even if a large body of clinical studies strongly suggests otherwise. The rift between retail optometry and clinical optometry science has never really been addressed (some say this is mainly since no commercially viable product has been found to justify such reconciliation).
And yet here is Coopervision, a 1.8 billion dollar a year in sales behemoth of the optometry industry, directly and unquestionably implying it: focal planes, and by direct implication, hyperopic defocus, cause high myopia. Or to be more accurate, they are saying that myopic defocus will prevent the progression of myopia otherwise caused by hyperopic defocus.
There is little room in the business for discussing the realities of myopia control, as most are busy either selling a product or another (bills to pay retail optometry), or publishing studies that no-one on the retail level will ever read (publish or perish academia).
Maybe this is why this thundering entry into the myopia control field is making nary a sound in mainstream news.
This, a bit of a long topic. If you prefer to watch a more informal video rant / explainer, click over to our Youtube channel and MiSight video:

Captain Graybeard tells it how it is.
But Coopervision goes even further than the momentous claim of focal planes being able to control myopia progression, and their admission of eye diseases such as glaucoma and retinal detachment being a directly associated risk factor of myopia (something you won’t hear most retail optometrists tell you).
Here’s more Coopervision claims:
“May improve the self-esteem of children and teenagers”
Here again, an obvious one if you read endmyopia, but something retail optometry won’t talk about. There’s direct correlation between high myopia and emotional well-being.
Of course until there is commercial motivation, you rarely will hear the truth about health. But here it is, commercial motivation via MiSight, and alas, the truth.
Take a moment to marvel at all the cats being let out of the bag here, by Coopervision. You’ve got focal planes playing a crucial role in high, over 6 diopter myopia. You have other vision related complications such as glaucoma and retinal detachment, a direct consequence of myopia. You have emotional side effects of myopia.
If Coopervision wasn’t an 800 pound gorilla, there’d be license-to-practice withdrawal and court proceedings silencing all this talk.
But we’re still not done!
Coopervision takes stabs at all the darlings of commercial myopia control, things that have not been said by commercial entities. Take a look at their atropine statement:
Alternative: Atropine Risks
“Atropine has been shown to slow down the rate of progression of myopia however it has side effects including photophobia and reduced accommodation as well as long term safety concerns².”
Big deal here, again. Photophobia and reduced accommodation are serious side effects, impairing vision more seriously than myopia. Do you want to take a treatment which side effects worse than the original condition?
Ask any optometrist who prescribes atropine, and see if you’ll get this level of truth. You won’t.
And shockingly, Coopervision is still not done. They’re also taking direct shots at the other darling of commercial myopia control, Ortho-K:
Alternative: Ortho-K Risks
“Ortho-K was originally developed to control refractive error however it is believed flattening the central cornea induces an effective peripheral power profile that may control eye growth. Disadvantages of Ortho-K include discomfort and increased risk of infections; it’s also complex requiring specific fitting and management skills³.”
This too, straight from the MiSight marketing materials.
Do you want to risk eye infections? Yes, Coopervision are taking it easy on Ortho-K, about which far worse things could be said.
But they are saying it … both atropine and Ortho-K are far less effective than using focal plane changes, in particular 2 diopters of myopic defocus, to control myopia progression and entirely prevent high myopia. This until now has been entirely in the realm of the unspeakable on the mainstream optometry front, things you’d only read in dusty clinical studies or hear from by marginal outlets such as endmyopia here.
All this big talk of course, still begs the question:
How Effective is MiSight?
Studies are still in progress, outcomes unknown.
Since we do know (from clinical science) that defocus indeed controls axial length of the human eyeball (and with it myopia degree), it’s safe to say that MiSight will likely have a more positive impact than simple single focal plane corrections.
Lacking here of course is positive stimulus, which would help to further reduce the risks of myopia development – but that’s taking things quite a bit further than even Coopervision is willing to go.
All this leaves the question:
Why Isn’t Everyone Talking About MiSight?
And that’s where we get to why things are what they are.
Change in mainstream treatment happens slowly. You have to have a workforce of sales people out in the field, selling your product to individual optometrists. It’s no different from pharma, where the success of any given treatment significantly depends on the marketing dollars and direct sales efforts put in place. And even then, convincing an optometrist to switch treatments (at best), or start looking at myopia control (more realistically), is an uphill battle.
Profit is in serving a large number of customers, selling glasses and lenses. If you get into myopia control discussions, you:
1) Significantly increase the time spent per customer, and thereby reduce revenue opportunity per hour/day.
2) Dealing with education rather than simple symptom management also increases the risk of dissatisfaction from confused customers, the risk of making promises that may create expectations which are difficult to manage, and
3) return visits for support related questions, not yielding more sales.
None of this is attractive to the volume-focused optometry profession of today.
Less product penetration into the market means less marketing dollars, means less potential spending to have journalists cover this type of treatment. It is also a fundamentally complex technical proposition, since educating a reader base about things like focal planes and myopia development isn’t easily accomplished – at least not without the risk of loosing reader attention. How many people do you think would read an article like this one, even if it was filled with illustrations and quotes and big adjectives and promises?
And there we have it. A very interesting achievement by a large optometry focused corporation, bold claims, a potential step in the right direction – all of it muddied by the complex realities of commercial incentives, demands of the market place, and general apathy towards more involved but ultimately more rewarding solutions for myopia control.
Bravo to Coopervision for putting out an innovative product, with equally innovatively science reality based claims.
Check out the video rant of this topic too, if you haven’t yet: Coopervision MiSight, take by Jake.
*credit for finding this one, and original post by Despina
Cheers,
-Jake